
The World Health Organization has sounded a critical alert. Two months after the declaration of the Ebola epidemic in the Democratic Republic of Congo, official figures released on July 15 indicate over 2,000 cases, including 796 deaths. Yet, the organization warns that the actual number of infected individuals could be two to four times higher. What accounts for such a significant discrepancy? Why is this outbreak proving so challenging to control? Could the launch of a first-ever post-exposure prophylaxis clinical trial in Bunia this week shift the trajectory of this crisis?

Underreporting or systemic gaps?
The gap between reported cases and WHO’s estimates suggests either severe underreporting or systemic gaps in detection. Remote communities, limited healthcare access, and ongoing insecurity in eastern DRC complicate surveillance and response efforts. Travel restrictions and community mistrust further hinder containment, as families often conceal symptoms to avoid stigmatization or quarantine.
With over 796 lives already lost, the situation demands urgent action. The discrepancy in figures raises questions about data accuracy and the true scale of transmission. Are we witnessing a silent spread beyond official records?
Bunia’s clinical trial: a potential turning point
This week, health authorities launched a groundbreaking clinical trial in Bunia aimed at testing a post-exposure prophylaxis (PEP) regimen. This experimental approach involves administering treatment to individuals exposed to the virus to prevent infection. If successful, it could offer a new strategy to curb transmission and protect at-risk populations.
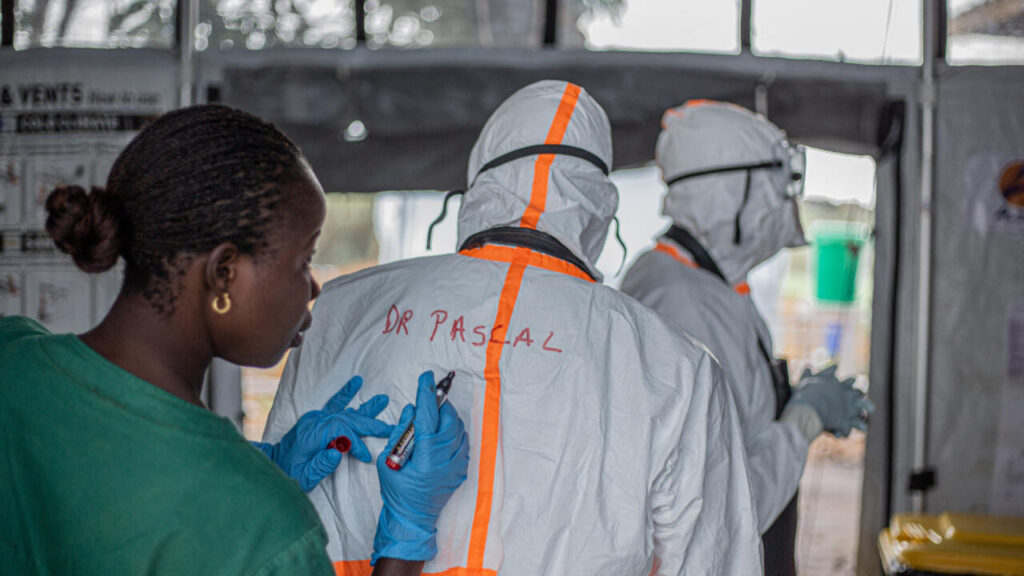
The trial comes as health workers face mounting challenges, including limited resources, logistical barriers, and persistent insecurity. Success hinges on community engagement, trust-building, and rapid deployment of medical teams.
Key challenges in containing Ebola
- Geographical barriers: Remote and conflict-affected regions like Ituri and North Kivu hinder access to healthcare facilities.
- Community resistance: Fear and misinformation lead to avoidance of treatment centers and concealment of cases.
- Healthcare strain: Overburdened facilities struggle to manage patient loads and maintain infection control protocols.
- Logistical hurdles: Supply chains for vaccines and treatments face delays due to insecurity and infrastructure gaps.
What’s next?
The clinical trial in Bunia represents a critical step forward. However, long-term control depends on strengthening surveillance, improving community trust, and ensuring equitable access to care. Without these, the epidemic may continue to simmer beneath the surface, undetected and unchecked.
You may also like
-
Us issues highest travel warning for Sahel alliance nations amid terror surge
-
Unlocking Benin’s entrepreneurial potential through sme and artisan support
-
Benin’s digital transformation vision unveiled at CAFRAD forum in Rabat
-
Tchad to lift african visas in 2027 for seamless travel
-
Côte d’Ivoire embassy in France launches strong protest over Jean-Luc Mélenchon’s remarks